Locations
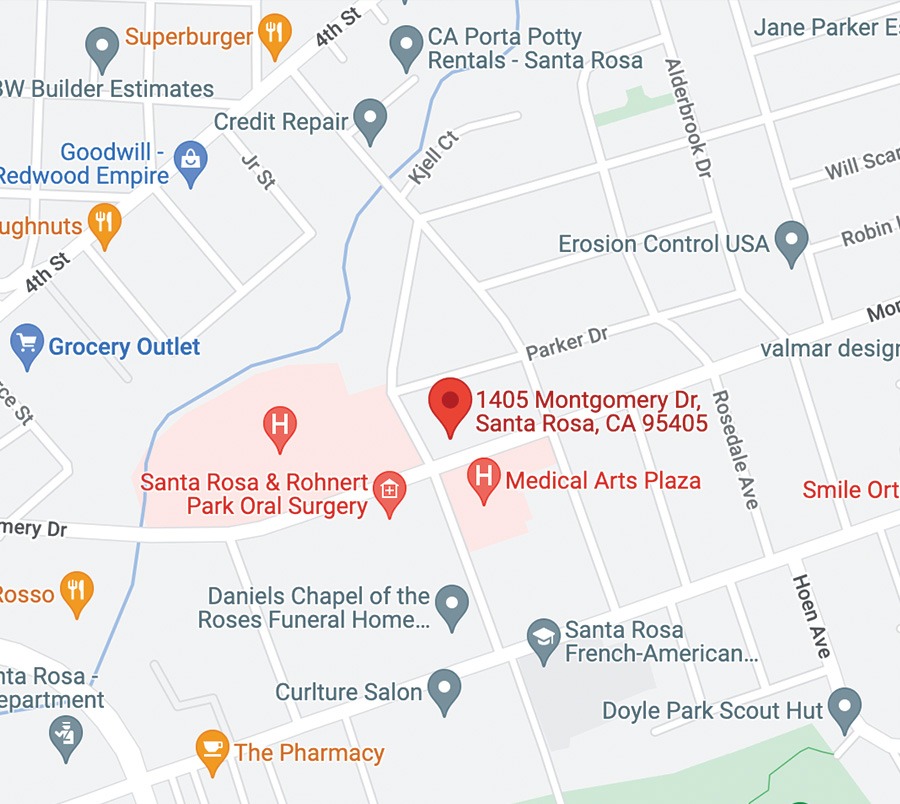
Santa Rosa, Montgomery Dr.
We Keep You
in Motion.
Monday to Friday
8:00 am. to 5:00 pm.
Appointments
Privacy Policy
Santa Rosa Orthopaedics
© Copyright . All Rights Reserved.
Locations
New building under construction.
Privacy Policy
Santa Rosa Orthopaedics © Copyright . All Rights Reserved. Website maintained by Durling Digital